

The purpose of the present study was to evaluate the role of whole-spine screening using short tau inversion recovery (STIR) or fat-suppressed T2W fast spin echo (FSE) sequences in patients with spinal tuberculosis (TB).
The identification of noncontiguous multiple-level spinal tuberculosis (NMLST), symptomatic or not, is important because of its management implications. Most centers do not perform routine whole-spine magnetic resonance imaging (MRI), and the reported incidence of NMLST varies from 1.1% to 74.1%.
Materials and Methods
Patients
We completed a retrospective review of clinical and radiographic data that were prospectively collected on 365 patients with spinal TB who were diagnosed and treated at Jawaharlal Nehru Medical College Hospital, Aligarh, from January 2010 to January 2015. The ethical committee of the Jawaharlal Nehru Medical College Hospital approved the study and informed consent was waived. Inclusion criteria included available whole-spine MRI performed on admission and confirmation of vertebral TB by histology, microbiology, or positive response to anti-tubercular treatment.
Diagnosis
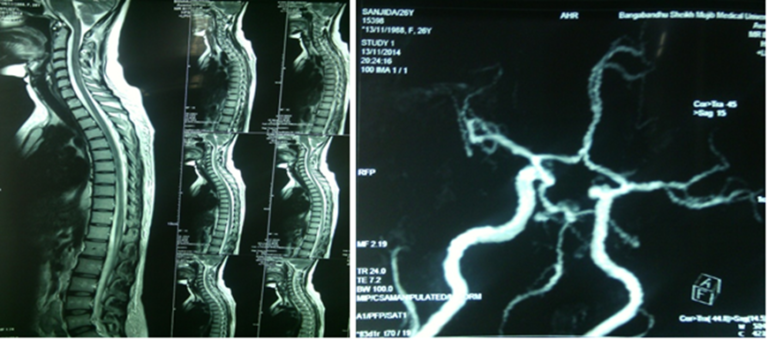
Diagnosis was confirmed after open surgical biopsy or image-guided percutaneous needle biopsy by histology or microbiology. Histological evaluation of biopsy samples was performed to look for granulomas, Langhans giant cells, and caseous necrosis. Microscopic examination was performed to check for acid-fast bacilli. Specimens were cultured for a total of 6 weeks before being declared negative. For patients where a tissue confirmation of TB was not available, a positive response to anti-tubercular treatment was considered diagnostic. The MRI protocol varied among patients but for the most part included the following pulse sequences: T1W, T2W in the sagittal plane, STIR in the coronal plane, and axial T1W and T2W. Post-contrast fat-suppressed T1W images were obtained in three orthogonal planes.